

As melanoma and NMSC skin cancers are often identifiable to the naked eye, skin self-examinations by patients and total-body skin examinations by physicians can lead to earlier detection and a reduction in mortality.[1][2]
Mass screening involves testing across an apparently healthy population in order to identify the early stages of disease in individuals.[3] Currently, population-based screening is not recommended for melanoma or other skin cancers, due to insufficient evidence that it reduces mortality.[4]
Individuals who are concerned about skin cancer or changes in their skin should seek advice from a medical practitioner and discuss their skin cancer risk and need for medical checks or self-examination.
Skin self-examination
In 2018 the US Preventive Task Force cited insufficient evidence to be able to assess the benefits of skin self-examination.[5] Cancer Council Australia recommends skin self-examination for those at elevated risk of skin cancer, particularly for those over 40 years of age, outdoor workers, and those with a personal or family history of skin cancer.[6]
Early detection through skin self-examination potentially reduces the risk of advanced melanoma by 63% through early detection of thinner lesions.[2] It is also associated with increased detection of ≤1mm thick lesions,[7] which have a high 95% five-year survival.[1] The 10-year survival rate for thin invasive melanomas (specifically non-ulcerated level II lesions) is 99% in those younger than 60 years.[8]
A Queensland study found nearly half (44%) of those with histologically confirmed melanoma detected the melanoma themselves.[9]
High risk individuals are encouraged to regularly check all areas of their skin (including areas not typically exposed to the sun) for suspicious spots/moles (naevi) and to look for changes in shape, colour or size of existing pigmented lesions.[6][4] Individuals concerned about their skin cancer risk, or new or changing skin lesions, should seek advice from a medical practitioner.[6]
Characteristics of suspicious spots/moles are described by 'ABCD[4]E':
- Asymmetry,
- Border irregularity,
- Colour: variable (including a surrounding coloured halo)
- Diameter >6 mm
'E' is also often used to represent ‘Evolving’.[10]
In clinical settings, ‘EFG’ is additionally used to refer to characteristics of Nodular melanoma (a subtype with a much poorer prognosis). In this case, E stands for Elevated, while F represents firm and G represents Growing over the past month.[4]
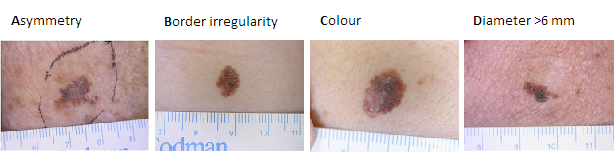
Figure 1: 'ABCD' characteristics
Images generously provided by Dr Alvin Chong, Skin & Cancer Foundation Victoria
A general sense of abnormality compared with an individual’s other pigmented lesions can also be a sign of a cancerous lesion - the so-called “ugly duckling” effect.[4][11]

Figure 2: “Ugly duckling” pigmented lesion
Image generously provided by Dr Alvin Chong, Skin & Cancer Foundation Victoria
Additional 'ABCD' criteria have been proposed for diagnosing paediatric melanomas based on a retrospective study which found that 60% of children under 10 years of age and 40% of 11-19 year-olds did not present with typical 'ABCDE' clinical presentation. Cordoro and colleagues recommend using the conventional 'ABCDE' criteria along with the additional criteria to facilitate diagnosis[12]:
- Amelanotic (lesions that are red or pink)
- Bleeding and bump (bleeding and raised lesions)
- Colour uniformity
- De novo development and diameter <6mm
The Royal Australian College of General Practitioners recommend that high-risk individuals (those with >5 dysplastic naevi and a personal history of melanoma/history in a first-degree relative) self-examine every 3 months, and may benefit from self-photography.[4]
The 2013-14 National Health Survey of more than 19,000 Australians estimated that two-thirds (66%) of Australians regularly check their skin for changes in freckles and moles.[13] A 2017 survey by The Skin and Cancer Foundation found that of the 1,000 people surveyed, 70% of women and 64% of men self-check their skin for disease, including skin cancer.[14]
Mass screening
Mass screening for the general adult population was not recommended in 2016 by the US Preventative Services Task Force for the early detection of cutaneous melanoma, basal cell carcinoma, or squamous cell carcinoma.[15] The task force concluded that there was “insufficient evidence to assess the balance of benefits and harms of visual skin examination by a clinician to screen for skin cancer in adults”. A study by Aitken and colleagues has found that clinical whole-body skin examination leads to detection of melanoma tumours at an earlier stage (when the tumour is thinner),[16] which in turn reduces mortality.[1] However the study does not provide information on the costs to the health system.
Skin cancer does not meet population screening guidelines as defined by the World Health Organization[17] due to a lack of high level evidence showing a reduction in mortality, and a low mortality rate for non-melanocytic skin cancers (NMSC),[15]
In addition, diagnostic accuracy for melanoma is modest and there is limited and inconsistent evidence of diagnostic accuracy of NMSC through clinical visual skin examination.[15] Therefore, Cancer Council Australia's current recommendation include opportunistic screening and skin self-examination in place of routine population screening.[6]
Diagnosing skin cancer
Dermatoscopy

Figure 3: Dermatoscopes
Image generously provided by Dr Alvin Chong, Skin & Cancer Foundation Victoria
Naked-eye clinical diagnosis of cutaneous melanoma has an accuracy rate of only 60%.[18] Therefore dermatoscopy, also known as dermoscopy, (examining lesions using a hand-held microscope) is used in order to improve accuracy in diagnosing pigmented skin lesions[19] and unpigmented lesions.[20] Dermatoscopy has an accuracy of 89% and sensitivity of 82.6% for detecting melanocytic lesions, a sensitivity of 98.6% for basal cell carcinoma and 86.5% for squamous cell carcinoma. Improvement in sensitivity with use of dermatoscopy was higher for melanocytic than non-melanocytic lesions.[21]
The number needed to treat (NNT) is an epidemiological measure used in assessing the effectiveness of a healthcare intervention − in this case a rate of excised melanomas to misdiagnosed benign lesions. Lower numbers needed to treat (NNT) signify a lower rate of misdiagnosed benign lesions to melanomas excised, and therefore signify reduced morbidity and healthcare costs.[22]
A study by Rosendahl and colleagues found that there was an association between higher dermatoscopy use and lower melanoma numbers need to treat (NNTs), indicating fewer misdiagnoses among general practitioners using dermatoscopes. However, after adjusting by practice type (dedicated skin cancer practitioner, general practitioner (GP), GP with a special interest in skin cancer) these were no longer significant.[23] This result may be explained in light of a review that found diagnostic accuracy via dermatoscopy significantly depends on the examiner’s degree of experience and training.[24]
Dermoscopy is more accurate when interpreted with the patient present rather than using dermoscopy images. Data to support its use in primary care are limited, however it may assist general practitioners to correctly identify people with suspicious lesions who need to be seen by a specialist.[24]
Primary care physicians
Within Australia, skin cancers are the most common cancer managed by general practitioners (GPs), who have historically been the first port of call for patients seeking an examination for skin cancer.[25] GPs are also responsible for the majority of skin cancer excisions, and are increasingly also performing surgical repairs (flap and graft repairs).[26] A study of Australian GPs showed higher diagnostic accuracy among GPs who specialised in skin cancer than GPs within a general practice.[23] However, an earlier study in Queensland reported similar levels of diagnosis accuracy among GPs whether they were working in a skin cancer clinic or not.[27]
Dermatoscopy use[23] and a physician’s level of experience with diagnosing skin cancer[27] have been shown to be the main factors determining diagnostic accuracy.
Skin cancer clinics
Historically, skin cancer management was performed primarily by general practitioners, but in recent years there has been a rapid increase in the number of skin cancer clinics.[25]
Overall, the majority of skin cancer excisions in Australia are performed by general practitioners.[26] In a study of surgeries performed between 2001-2005, GPs within a general practice performed more excisions of non-melanocytic skin cancers than GPs working in skin cancer clinics, who perform more melanoma excisions. However, melanoma excisions by GPs and skin cancer clinic GPs are similar in Queensland, where GPs have nearly double the national excision rate.[26]
Some concerns have been raised that skin cancer clinics are not accredited against a standard, and that they primarily employ general practitioners who have limited training, with no formal award course offered.[28] It has also been suggested that unnecessary excisions of spots/moles are frequent in skin cancer clinics.[29]
Overall, studies show that NNT in skin cancer clinics compare similarly between GPs in general and more specialised practices.[25][28] Further, diagnostic accuracy (sensitivity) is similar among skin cancer clinics and general practice.[27] However, diagnosis is just one aspect and research into other health outcomes for skin cancer clinics such as effectiveness of treatment and surgical repair are required to be able to fully evaluate Australian skin cancer clinics.[25]
Dermatologists
A comparison of multiple studies showed that in Australia, dermatologists have the lowest NNT (therefore lowest rate of misdiagnosis of benign lesions) as compared with general practitioners, doctors with a dedicated skin cancer practice, and doctors working in skin cancer clinics.[23]
A 2020 meta-analysis found that internationally, Pigmented lesion specialists have the lowest NNT, followed by dermatologists, then primary care physicians. The authors acknowledged that while geographic differences play a role, analysing all published data by clinical setting, irrespective of geography, gives the best estimation of NNT.[30]
Last modified: 30 June 2020
- Balch CM, Soong SJ, Atkins MB, Buzaid AC, Cascinelli N, Coit DG, et al. An evidence-based staging system for cutaneous melanoma. CA Cancer J Clin 2004 May;54(3):131-49; quiz 182-4 Available from: http://www.ncbi.nlm.nih.gov/pubmed/15195788.
- Berwick M, Begg CB, Fine JA, Roush GC, Barnhill RL. Screening for cutaneous melanoma by skin self-examination. J Natl Cancer Inst 1996 Jan 3;88(1):17-23 Available from: http://www.ncbi.nlm.nih.gov/pubmed/8847720.
- Wilson JM, Jungner YG. [Principles and practice of mass screening for disease]. Bol Oficina Sanit Panam 1968 Oct;65(4):281-393 Available from: http://www.ncbi.nlm.nih.gov/pubmed/4234760.
- The Royal Australian College of General Practitioners. Guidelines for preventive activities in general practice. 9th edn. East Melbourne, Australia; 2016.
- Grossman DC, Curry SJ, Owens DK, Barry MJ, Caughey AB, Davidson KW, et al. Behavioral Counseling to Prevent Skin Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2018 Mar 20;319(11):1134-1142 Available from: http://www.ncbi.nlm.nih.gov/pubmed/29558558.
- Cancer Council Australia. Position statement: Screening and early detection of skin cancer. Sydney, Australia: Cancer Council Australia; 2019 [cited 2020 Jun 18] Available from: https://www.cancer.org.au/about-us/policy-and-advocacy/position-statements/uv/early-detection.
- Carli P, De Giorgi V, Palli D, Maurichi A, Mulas P, Orlandi C, et al. Dermatologist detection and skin self-examination are associated with thinner melanomas: results from a survey of the Italian Multidisciplinary Group on Melanoma. Arch Dermatol 2003 May;139(5):607-12 Available from: http://www.ncbi.nlm.nih.gov/pubmed/12756097.
- Gimotty PA, Elder DE, Fraker DL, Botbyl J, Sellers K, Elenitsas R, et al. Identification of high-risk patients among those diagnosed with thin cutaneous melanomas. J Clin Oncol 2007 Mar 20;25(9):1129-34 Available from: http://www.ncbi.nlm.nih.gov/pubmed/17369575.
- McPherson M, Elwood M, English DR, Baade PD, Youl PH, Aitken JF. Presentation and detection of invasive melanoma in a high-risk population. J Am Acad Dermatol 2006 May;54(5):783-92 Available from: http://www.ncbi.nlm.nih.gov/pubmed/16635658.
- Abbasi NR, Shaw HM, Rigel DS, Friedman RJ, McCarthy WH, Osman I, et al. Early diagnosis of cutaneous melanoma: revisiting the ABCD criteria. JAMA 2004 Dec 8;292(22):2771-6 Available from: http://www.ncbi.nlm.nih.gov/pubmed/15585738.
- Grob JJ, Bonerandi JJ. The 'ugly duckling' sign: identification of the common characteristics of nevi in an individual as a basis for melanoma screening. Arch Dermatol 1998 Jan;134(1):103-4 Available from: http://www.ncbi.nlm.nih.gov/pubmed/9449921.
- Cordoro KM, Gupta D, Frieden IJ, McCalmont T, Kashani-Sabet M. Pediatric melanoma: results of a large cohort study and proposal for modified ABCD detection criteria for children. J Am Acad Dermatol 2013 Jun;68(6):913-25 Available from: http://www.ncbi.nlm.nih.gov/pubmed/23395590.
- Australian Bureau of Statistics. 4364.0 National Health Survey: Health Service Usage and Health Related Actions, Australia, 2013-14. Canberra, Australia: Australian Bureau of Statistics; 2017 Available from: https://www.abs.gov.au/AUSSTATS/abs@.nsf/Lookup/4364.0.55.002Main+Features12014-15?OpenDocument.
- Skin & Cancer Foundation Inc. Skin Health Australia Report Card 2017. Melbourne, Australia: Skin & Cancer Foundation Inc; 2017 [cited 2020 Jun 15] Available from: https://skincancer.blob.core.windows.net/assets/uploads/files/SHARC%20REPORT/2017.SHARC/2017.SHARC.Report_s2.pdf.
- Bibbins-Domingo K, Grossman DC, Curry SJ, Davidson KW, Ebell M, Epling JW Jr, et al. Screening for Skin Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2016 Jul 26;316(4):429-35 Available from: http://www.ncbi.nlm.nih.gov/pubmed/27458948.
- Aitken JF, Elwood M, Baade PD, Youl P, English D. Clinical whole-body skin examination reduces the incidence of thick melanomas. Int J Cancer 2010 Jan 15;126(2):450-8 Available from: http://www.ncbi.nlm.nih.gov/pubmed/19609948.
- World Health Organization. Screening for various cancers. Geneva, Switzerland; 2008 Available from: www.who.int/cancer/detection/variouscancer/en/.
- Kittler H, Pehamberger H, Wolff K, Binder M. Diagnostic accuracy of dermoscopy. Lancet Oncol 2002 Mar;3(3):159-65 Available from: http://www.ncbi.nlm.nih.gov/pubmed/11902502.
- Campos-do-Carmo G, Ramos-e-Silva M. Dermoscopy: basic concepts. Int J Dermatol 2008 Jul;47(7):712-9 Available from: http://www.ncbi.nlm.nih.gov/pubmed/18613881.
- Sinz C, Tschandl P, Rosendahl C, Akay BN, Argenziano G, Blum A, et al. Accuracy of dermatoscopy for the diagnosis of nonpigmented cancers of the skin. J Am Acad Dermatol 2017 Dec;77(6):1100-1109 Available from: http://www.ncbi.nlm.nih.gov/pubmed/28941871.
- Rosendahl C, Tschandl P, Cameron A, Kittler H. Diagnostic accuracy of dermatoscopy for melanocytic and nonmelanocytic pigmented lesions. J Am Acad Dermatol 2011 Jun;64(6):1068-73 Available from: http://www.ncbi.nlm.nih.gov/pubmed/21440329.
- Argenziano G, Cerroni L, Zalaudek I, Staibano S, Hofmann-Wellenhof R, Arpaia N, et al. Accuracy in melanoma detection: a 10-year multicenter survey. J Am Acad Dermatol 2012 Jul;67(1):54-9 Available from: http://www.ncbi.nlm.nih.gov/pubmed/21982636.
- Rosendahl C, Williams G, Eley D, Wilson T, Canning G, Keir J, et al. The impact of subspecialization and dermatoscopy use on accuracy of melanoma diagnosis among primary care doctors in Australia. J Am Acad Dermatol 2012 Nov;67(5):846-52 Available from: http://www.ncbi.nlm.nih.gov/pubmed/22325462.
- Dinnes J, Deeks JJ, Chuchu N, Ferrante di Ruffano L, Matin RN, Thomson DR, et al. Dermoscopy, with and without visual inspection, for diagnosing melanoma in adults. Cochrane Database Syst Rev 2018 Dec 4;12:CD011902 Available from: http://www.ncbi.nlm.nih.gov/pubmed/30521682.
- Wilkinson D, Askew DA, Dixon A. Skin cancer clinics in Australia: workload profile and performance indicators from an analysis of billing data. Med J Aust 2006 Feb 20;184(4):162-4 Available from: http://www.ncbi.nlm.nih.gov/pubmed/16489899.
- Askew DA, Wilkinson D, Schluter PJ, Eckert K. Skin cancer surgery in Australia 2001-2005: the changing role of the general practitioner. Med J Aust 2007 Aug 20;187(4):210-4 Available from: http://www.ncbi.nlm.nih.gov/pubmed/17708722.
- Youl PH, Baade PD, Janda M, Del Mar CB, Whiteman DC, Aitken JF. Diagnosing skin cancer in primary care: how do mainstream general practitioners compare with primary care skin cancer clinic doctors? Med J Aust 2007 Aug 20;187(4):215-20 Available from: http://www.ncbi.nlm.nih.gov/pubmed/17708723.
- Wilkinson D, Bourne P, Dixon A, Kitchener S. Skin cancer medicine in primary care: towards an agenda for quality health outcomes. Med J Aust 2006 Jan 2;184(1):11-2 Available from: http://www.ncbi.nlm.nih.gov/pubmed/16398623.
- Hansen C, Wilkinson D, Hansen M, Argenziano G. How good are skin cancer clinics at melanoma detection? Number needed to treat variability across a national clinic group in Australia. J Am Acad Dermatol 2009 Oct;61(4):599-604 Available from: http://www.ncbi.nlm.nih.gov/pubmed/19664848.
- Petty AJ, Ackerson B, Garza R, Peterson M, Liu B, Green C, et al. Meta-analysis of number needed to treat for diagnosis of melanoma by clinical setting. J Am Acad Dermatol 2020 May;82(5):1158-1165 Available from: http://www.ncbi.nlm.nih.gov/pubmed/31931085.